Ultrasonic examination & computed tomography examination of endoleak after endovascular aortic aneurysm repair
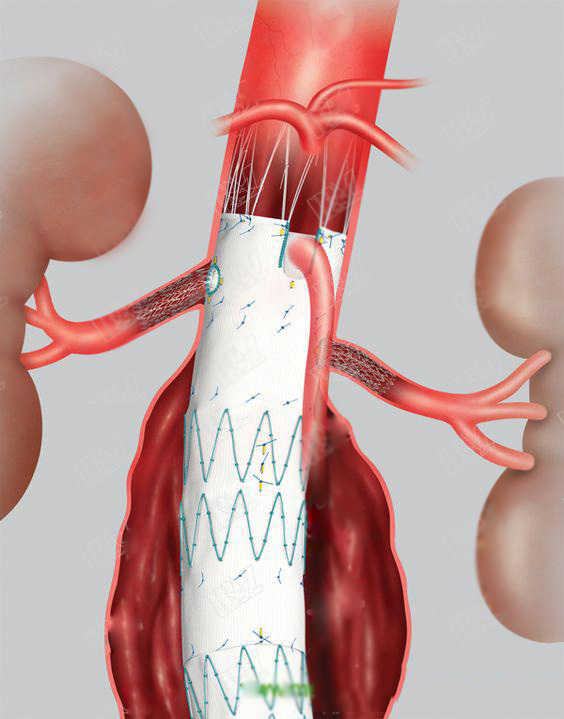
Abdominal Aortic Aneurysm (AAA) is a local swelling or enlargement of blood vessels that carry blood to the abdomen (stomach), pelvis and leg. AAA patients risk of sudden death due to AAA rupture (burst). Once detected, it is advisable to intervene (treat) once the AAA diameter is greater than about 5 cm. Most repairs are now performed using new vascular linings within an aneurysm guided by X-ray control (Endovascular Aneurysm Repair or EVAR).
Once the new lining is in place, the seals on both ends may leak, or the blood vessel branches caused by the aneurysmal wall may seep into the AAA sac. These are collectively referred to as internal leakage. Common internal leakage after EVAR, about 40% of people during the development of monitoring (follow-up). Internal leakage may be related to ruptured advanced aneurysm, so testing and monitoring are essential.
Ultrasound (using high frequency sound waves), computed tomography (using X-rays), and magnetic resonance scanning (using strong magnetic fields and radio waves) have been used to detect and monitor internal leaks. Dyes (contrast media) are sometimes injected into veins to improve the accuracy of ultrasound (contrast-enhanced ultrasound).
One survey showed significant individual effects based on statistically significant years of publication and study quality for individuals based on the CDUS study. In studies published prior to 2006, the sensitivity estimate was higher than the research plan published in 2006 or later (P <0.001); and the studies judged as low / unclear provided a higher sensitivity estimate. When regression testing was applied to a person-based CE-CDUS study, none of the items (ie, the direction, quality, and age at which the study was designed) were identified as a source of heterogeneity.
Twenty-two studies provided accuracy data based on the number of scans performed (four of which provided data on the use and non-use of contrast). Studies that provide scan-based data have shown similar results. The CDUS summary (18 studies) showed a sensitivity of 0.87 (95% CI 0.55 to 0.85), specificity of 0.95 (95% CI 0.90 to 0.96) and CE-CDUS% CI 0.71 to 0.96).
This review shows that these two modes of ultrasound (with or without contrast) show high specificity. For internal leakage, CE-CDUS seems to outperform CDUS. In an endovascular monitoring program, CE-CDUS can be introduced as a routine diagnostic modality followed by a CT scan to determine the type of endoleak and subsequent management of care only if the ultrasound is positive.
Call: 0086-138 2644 8637
E-mail: cindy@medicalequipment-msl.com



